
Folliculitis keloidalis — extra information
Introduction
Demographics
Causes
Clinical features
Variation in skin types
Complications
Diagnosis
Differential diagnoses
Treatment
Prevention
Outcome
What is folliculitis keloidalis?
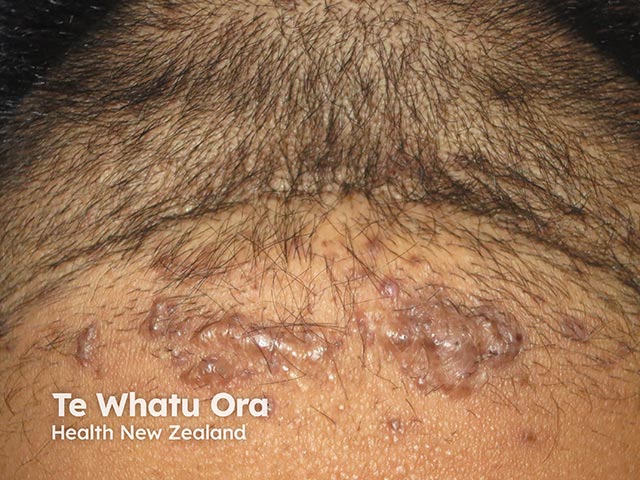
Folliculitis keloidalis, also called folliculitis keloidalis nuchae (FKN), is a chronic scarring folliculitis of the occipital scalp. It mostly affects men of African-Caribbean descent with black curly hair.
Folliculitis keloidalis is commonly called acne keloidalis nuchae (AKN), although the condition is not related to acne vulgaris, and the scars formed are not true keloid scars. Dermatitis papillaris capillitii is another synonym.




View more images of folliculitis keloidalis
Who gets folliculitis keloidalis?
Folliculitis keloidalis mostly affects men of African-Caribbean descent with afro-textured hair, and may also affect men of Hispanic, Middle Eastern, Mediterranean, Asian, and Pacific descent. It is 20 times more common in men than women.
Onset occurs after adolescence and is rare after the age of 55 years.
Folliculitis keloidalis may occur in combination with other inflammatory conditions such as acne inversa (hidradenitis suppurativa), dissecting scalp cellulitis, pilonidal disease, and acne conglobata.
What causes folliculitis keloidalis?
The exact pathophysiology of folliculitis keloidalis is poorly understood but is thought to be exacerbated by mechanical injury and an aberrant immune response. Potential contributing factors include:
- Skin injury — arising from very short haircuts, close shaving, or chronic trauma, such as friction from headgear or collars.
- Hair texture — more greatly associated with coarse, wiry, and tightly curled hair, which can predispose to ingrown hairs and folliculitis.
- Immune response
- Pathogenic immune theory posits that intrafollicular antigens (eg, skin flora, Demodex, sebum, or cosmetics) stimulate an inflammatory reaction at the isthmus of the pilosebaceous unit.
- This inflammatory response destroys the sebaceous gland and follicular wall, before progressing into the dermis and causing a follicular scar.
- Hypertrophic scarring eventually develops due to the hair shaft fragments and degenerating epithelial components in the dermis.
- Environmental factors — eg, heat and humidity.
- Medications and other substances — eg, ciclosporin, calcineurin inhibitor, carbamazepine, anabolic steroids, or whey protein supplements.
- Other factors — including excess androgen and seborrhoea.
Other disorders reported to be associated with folliculitis keloidalis include metabolic syndrome, gout, hidradenitis suppurativa, and keratosis follicularis spinulosa decalvans.
What are the clinical features of folliculitis keloidalis?
- Small itchy papules
- Located around the occipital scalp during early stages; can extend cranially towards the top as severity progresses.
- Occasionally, pustules around the hair follicles (folliculitis)
- Crusting or excoriation may be seen
- Scratching may lead to bacterial infection.
- Papules can congregate and enlarge to the point of being keloid-like scars.
- In advanced stages, scars can cause permanent hair loss (scarring alopecia) or suppurative abscesses.
- Hairless scars can form a band along the hairline.
- Tufted hairs may also be seen.
View images of folliculitis keloidalis
How do clinical features vary in differing types of skin?
The keloid-like scars may range from dark pink to dark brown or black in colour. Postinflammatory hyperpigmentation from papules and pustules is common in darker Fitzpatrick skin types (eg, III to VI).
What are the complications of folliculitis keloidalis?
- Secondary bacterial infection eg, from Staphylococcus aureus
- Draining sinus tracts
- Scarring alopecia
- Negative impacts on self-esteem
- Haircut-associated bleeding — can increase risk of infection and/or potential transmission of blood-borne diseases from shared barber equipment
How is folliculitis keloidalis diagnosed?
Folliculitis keloidalis is a clinical diagnosis based on the findings of papules, pustules, and keloid-like plaques on the occipital scalp and nape of the neck.
History
- A thorough history should be obtained from the patient, including:
- Age of onset of symptoms (post-puberty up to the fourth decade of life is typical) and rate of progression
- Pain or pruritus
- Exacerbating factors eg, close clipping or shaving
- Typical hairstyle and clothing choices
- Any prior treatments and how well they worked.
Examination
- Examine the entire scalp.
- Normally the area of disease is limited to the posterior scalp and nape.
- While folliculitis keloidalis can progress in a cranial direction, findings on other areas of the scalp should prompt consideration of differential diagnoses.
- Dermoscopy may reveal perifollicular pustules and a white halo around the hair follicles in early-stage disease. Late-stage disease may show tufted ‘doll hairs’.
Investigations
Biopsy is rarely necessary unless the diagnosis is equivocal. If there is uncertainty, consider a punch biopsy, ideally including a suspected keloidal papule and the base of the hair follicle. The histology of folliculitis keloidalis nuchae is characteristic, should a biopsy be performed.
Other investigations may be indicated depending on the differential diagnoses and/or suspected complications eg, fungal or bacterial culture.
What is the differential diagnosis for folliculitis keloidalis?
- Acne mechanica (frictional folliculitis)
- Bacterial folliculitis
- Molluscum contagiosum
- Tinea capitis (eg, kerion)
- Folliculitis decalvans (atypical cicatricial alopecia variant)
- Dissecting cellulitis of the scalp (atypical cicatricial alopecia variant)
- Lichen planopilaris
- Follicular cutaneous T-cell lymphoma
What is the treatment for folliculitis keloidalis?
Folliculitis keloidalis can be challenging to treat, and there are no consensus guidelines regarding management. Early diagnosis and intervention can help to prevent progression and reduce scarring and hair loss. The following measures may be helpful.
General measures
- Avoid picking, scratching, or rubbing the affected scalp.
- Change barbering habits to avoid short and razor haircuts.
- Minimise friction and irritation on the back of the neck eg, from headwear, sports gear, and high-collared shirts.
- Consider using an antimicrobial cleanser or shampoo to reduce secondary infection.
Specific measures
Mild to moderate cases:
- High-potency topical corticosteroids, often combined with topical retinoids (eg, adapalene, trifarotene, or tretinoin) — reassessing every 4–6 weeks and tapering once a good response is achieved (usually within 6–12 weeks)
- A topical antimicrobial (eg, clindamycin-benzoyl peroxide) is sometimes added if pustules are present.
Moderate to severe cases:
- Oral doxycycline can be trialled for at least 6–8 weeks, together with topical or intralesional corticosteroids, and/or topical retinoids.
If limited response to treatment (or extensive disease), consider:
- Escalating to oral isotretinoin
- Surgical excision, laser hair removal, laser resurfacing, or electrosurgery
- Other adjunctive therapies: UV light therapy or radiotherapy.
Secondary infection can complicate folliculitis keloidalis and may require additional antimicrobial therapy (guided by swab results). Intralesional corticosteroid administration is usually delayed until active bacterial infection is resolved.
How do you prevent folliculitis keloidalis?
While it isn’t known how to completely prevent folliculitis keloidalis in the first place, one of the key aims of management is to prevent disease progression by:
- Avoiding potential exacerbating factors through lifestyle and behavioural modification
- Treating keloidal scars early to prevent extension, confluent scarring, and hair loss.
What is the outcome for folliculitis keloidalis?
Folliculitis keloidalis should be treated early to ensure the best cosmetic outcome. If left untreated, the acneiform lesions may eventually converge and form large keloid-like scars, making treatment more challenging.
Bibliography
- Cruz SA, Stein SL. A review of sports‐related dermatologic conditions. Transl Sports Med. 2020;3(4):300–308. doi: 10.1002/tsm2.145. Journal
- Liebich C, Wergin VV, Schubert I, et al. Dermatoses in competitive athletes. Dtsch Z Für Sportmed. 2021;72(1):5–12. doi: 10.5960/DZSM.2020.466. Journal
- Mackay-Wiggan JM, Husain S. Acne keloidalis nuchae: Management. Last updated Oct 26, 2021. UpToDate. Accessed Sept 7, 2024. Available here
- Mackay-Wiggan JM, Husain S. Acne keloidalis nuchae: Pathogenesis, clinical manifestations, and diagnosis. UpToDate. Last updated Jul 3, 2024. Accessed Nov 4, 2023. Available here
- Miteva M. Folliculitis Decalvans. In: Hair Pathology with Trichoscopic Correlations. CRC Press; 2021.
- Ogunbiyi A. Acne keloidalis nuchae: prevalence, impact, and management challenges. Clin Cosmet Investig Dermatol. 2016;9:483–489. doi: 10.2147/CCID.S99225. Journal
- Shavit E, Cohen A, Zoller L, et al. The burden of gout in acne keloidalis nuchae—Insights from a population-based study. J Cosmet Dermatol. 2023;22(1):284–288. doi: 10.1111/jocd.15476. Journal
- Umar S, Sila CR. Acne keloidalis nuchae: A role for low-dose radiotherapy. JAAD Case Rep. 2021;13:90–93. doi: 10.1016/j.jdcr.2021.05.008. Article
- Yip L, Barrett TH, Harries MJ. Folliculitis decalvans and lichen planopilaris phenotypic spectrum: a case series of biphasic clinical presentation and theories on pathogenesis. Clin Exp Dermatol. 2020;45(1):63–72. doi: 10.1111/ced.13989. Journal
On DermNet
- Folliculitis keloidalis images
- Folliculitis keloidalis nuchae pathology
- Hair loss
- Folliculitis
- Acne and other follicular disorders
- Diagnosis of scalp rashes
- Topical steroids
- Topical retinoids
- Intralesional steroid injection
- Tetracyclines
- Laser therapy in skin of colour
Other websites
- Acne Keloidalis Nuchae — The Australasian College of Dermatologists