
Dermoscopy of other non-melanocytic lesions
Created 2008.
Learning objectives
- Describe dermoscopic features of pigmented and non-pigmented non-melanocytic lesions
Introduction
Dermoscopy is useful to distinguish pigmented non-melanocytic lesions from benign and malignant melanocytic lesions. There are specific features that help to distinguish these.
Careful observation has resulted in the description of the dermoscopy of many non-pigmented lesions as well, which may be sometimes helpful in diagnosis for an itchy rash.
Dermoscopy of vascular lesions
The dermoscopic features of haemangiomas or angiomas are:
- Widespread red-blue lacunes
- Red-bluish-black homogeneous areas
Reactive haemangioma or pyogenic granuloma has a distinct keratinised border or collarette. Vascular structures are usually present but there is no clear lacunar pattern. White linear 'rail lines' are often featured. It is not always possible to distinguish reactive haemangioma from amelanotic melanoma.
Cutaneous lymphatic malformation (formerly called lymphangioma circumscriptum) has yellowish lacunes, sometimes tinged with blood.
Kaposi sarcoma under polarised microsocopy is characterised by multicoloured rainbow pattern in association with bluish-red colour, scaling and small brown globules. The rainbow pattern is occasionally seen in melanoma and other skin lesions.
Dermoscopy of haemangiomas








Dermoscopy of haemorrhage
Haemorrhage can be distinguished from pigmentation due to melanin by the purple colour. On plantar surfaces (e.g. talon noir) it may appear to have a parallel ridge pattern of discolouration with peripheral reddish-black globules. It may be helpful to shave off the surface keratin – sometimes biopsy is necessary to rule out melanoma.
Blood on dermoscopy







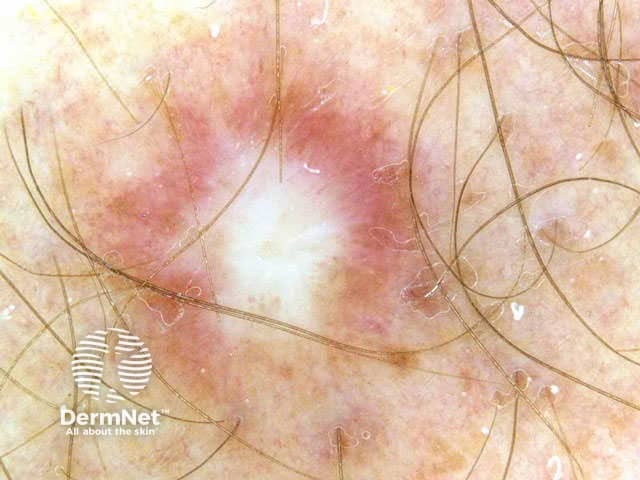
Dermoscopy of dermatofibroma
The dermatofibroma (also known as histiocytoma) is usually easy to diagnose clinically because of a firm fibrous consistency and surface dimpling on compression. Typically, dermoscopy of a dermatofibroma shows a faint network or pseudonetwork surrounding a pale amorphous area. Sometimes the central white area has white lines and brown holes (negative network). Chrystalline structures, i.e. white shiny lines, are commonly seen on polarised dermoscopy of dermatofibroma.
Haemosiderotic dermatofibroma (uncommon) is composed of numerous small vessels, extravasated erythrocytes and intra- and extracellular haemosiderin deposits. Dermoscopy reveals multicomponent pattern with a central bluish or reddish homogeneous area in combination with white or yellowish structures and a peripheral delicate pigment network.
Rarely, a rainbow pattern may be observed,




Dimpling sign (dermatofibroma)



Dermoscopy of neurofibroma
The common type of solitary neurofibroma is often clinically misdiagnosed as dermal naevus or skin tag. They are soft to firm papules or nodules. The buttonhole sign is helpful: you can push the lesion through a defect in the dermis and it bounces back when pressure is removed.
Dermoscopy reveals a featureless nodule.




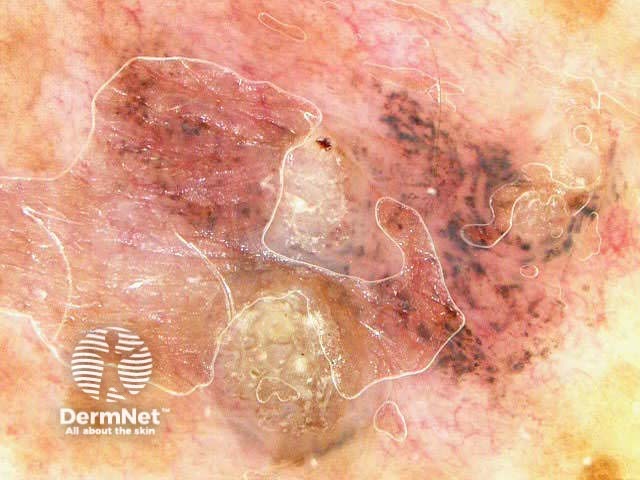
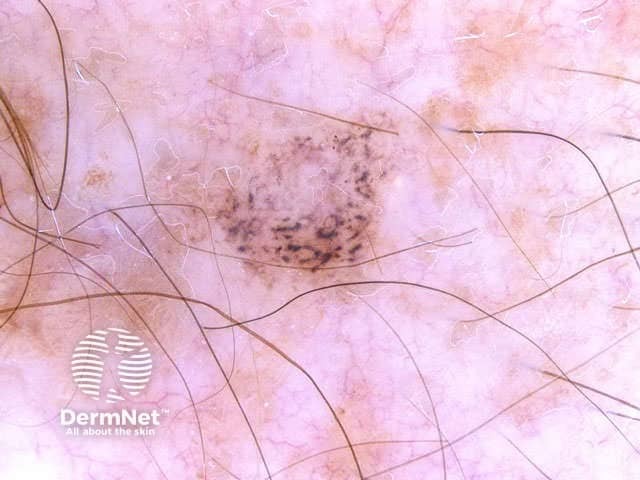
Dermoscopy of lichenoid keratosis
Lichenoid inflammation affecting a solar lentigo or seborrhoeic keratosis typically results in localised destruction of melanocytes and free melanin in the dermis or melanin within melanophages. These appear as granular areas of grey dots. Grey dots can also be typically seen within melanoma. However the lichenoid keratosis has no pigment network and there are usually amorphous areas with or without keratinous surface /or other features of seborrhoeic keratosis.
Dermoscopy of lichenoid keratosis: yellow arrows show grey dots


Dermoscopy of porokeratosis
Porokeratosis is distinguished by a cornoid lamella around the lesion. Sometimes there is prominent follicular plugging



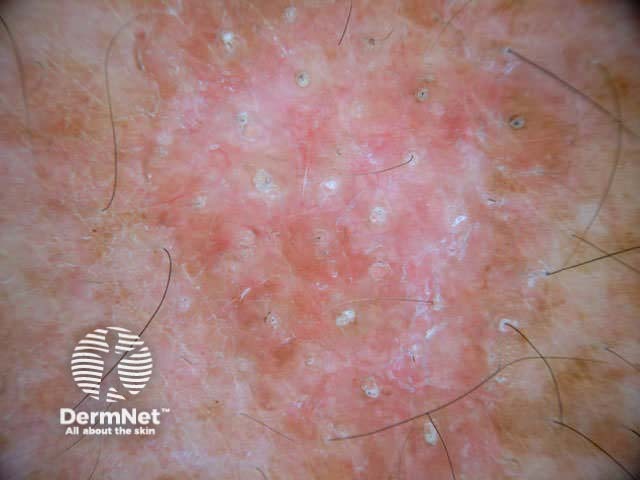
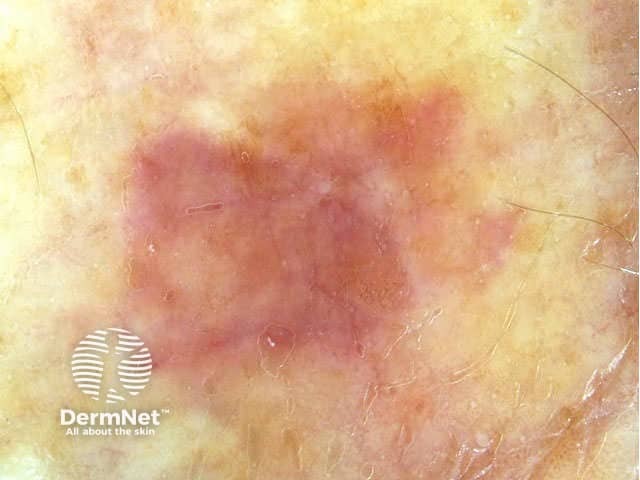
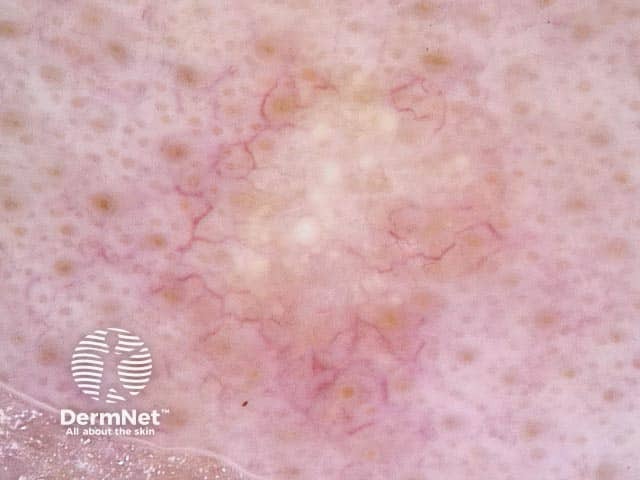
Dermoscopy of sebaceous hyperplasia
Sebaceous hyperplasia is distinguished by pale yellow lobules around a central follicular opening. Telangiectasia is common but tends to be uniform, in contrast to the irregular arborising vessels seen in basal cell carcinoma.

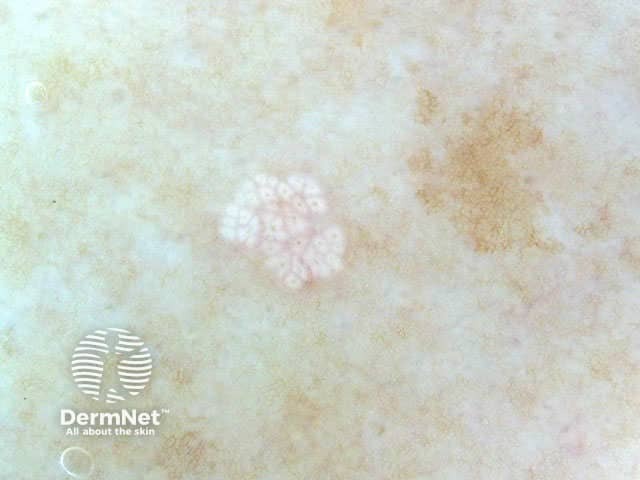
Dermoscopy of viral warts
Viral warts are keratinocytic lesions with a lobular structure (like frog spawn), sometimes with a central thrombosed capillary within each lobule. The normal dermatoglyphics are interrupted. Some have a papilliform structure.
In contrast, a corn has a translucent central core, and a callus is hyperkeratotic without other distinguishing features.



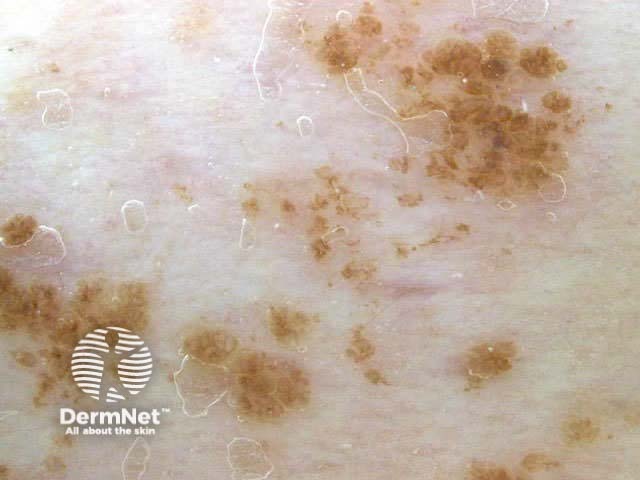
Dermoscopy of epidermal naevus
An epidermal naevus resembles a seborrhoeic keratosis or viral wart, with fissures, crypts and milia. However it is very uniform in appearance and appears within the first decade.

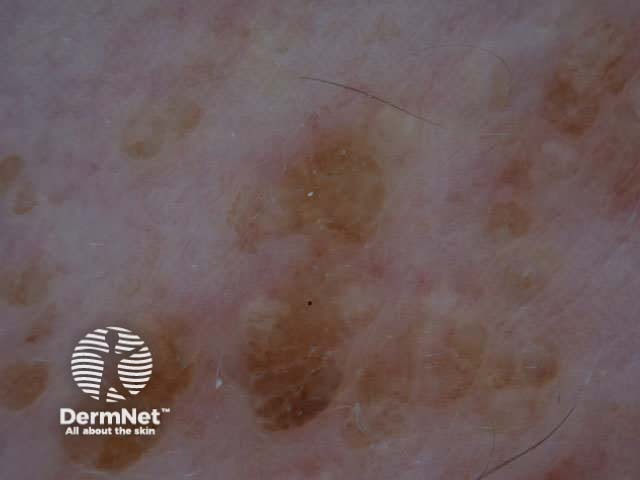
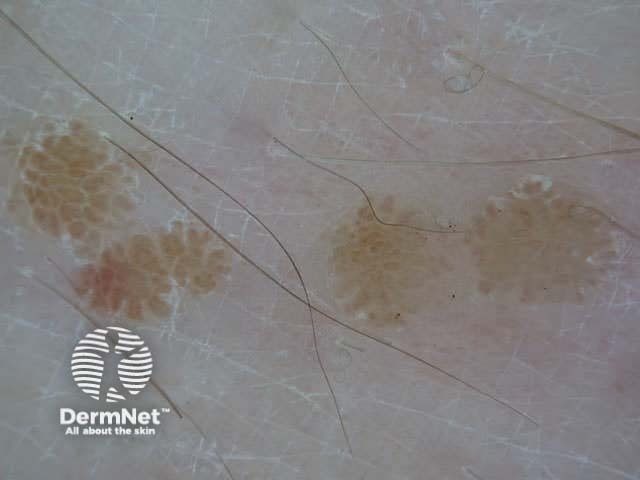
Dermoscopy of nipple
The areola and nipple are usually clinically obvious of course. However, an accessory nipple (present in 1 in 18 individuals) may resemble a compound naevus. Characteristically, the breast tissue has a delicate uniform peripheral pigment network.




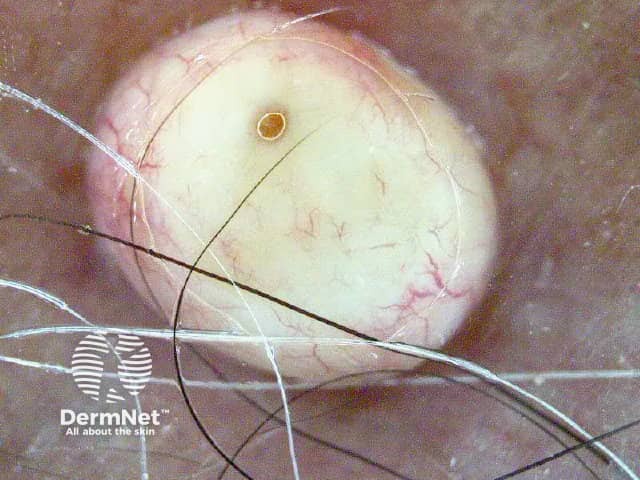
Dermoscopy of cysts
Close inspection of a cyst will show the follicular opening.


Dermoscopy of clear cell acanthoma
The clear cell acanthoma is an unusual benign epidermal tumour with characteristic dermoscopic features. There are multiple pinpoint or dotted vessels arranged in line like a string of pearls.




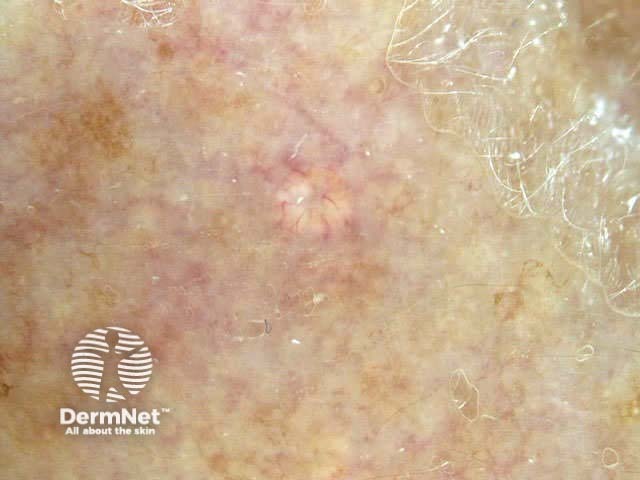
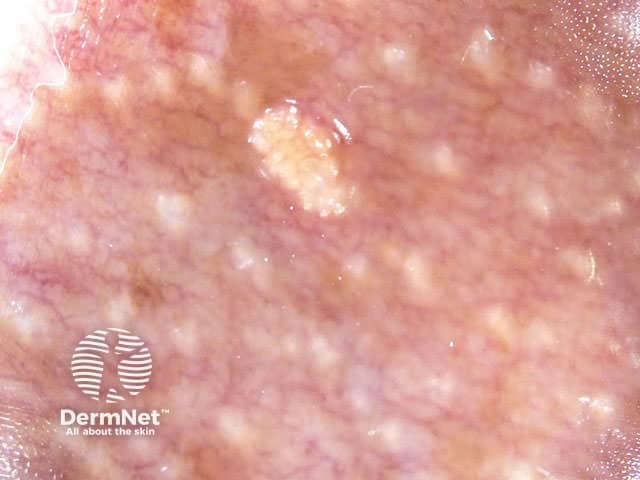
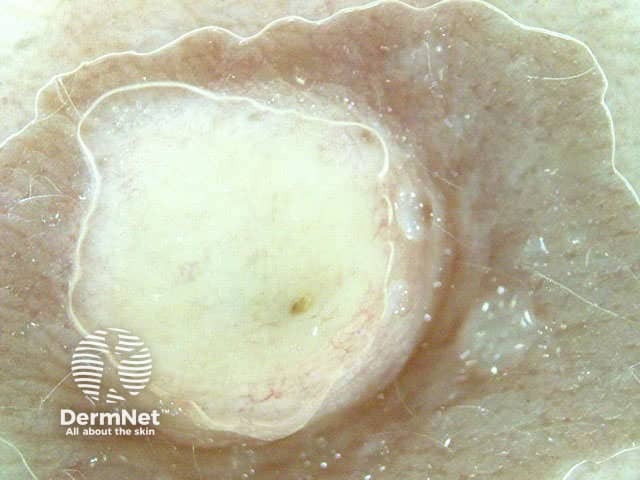
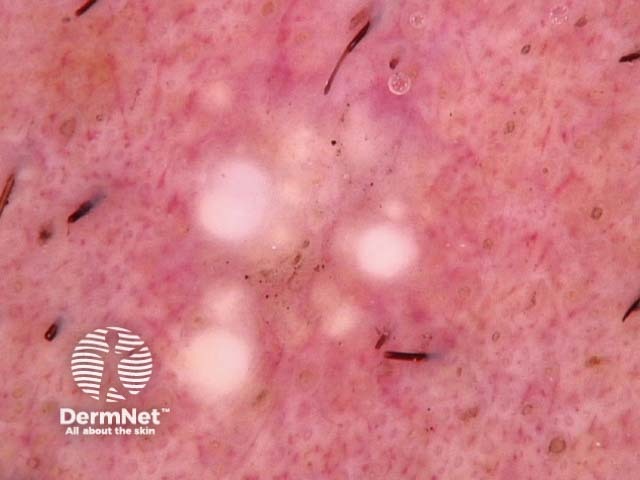
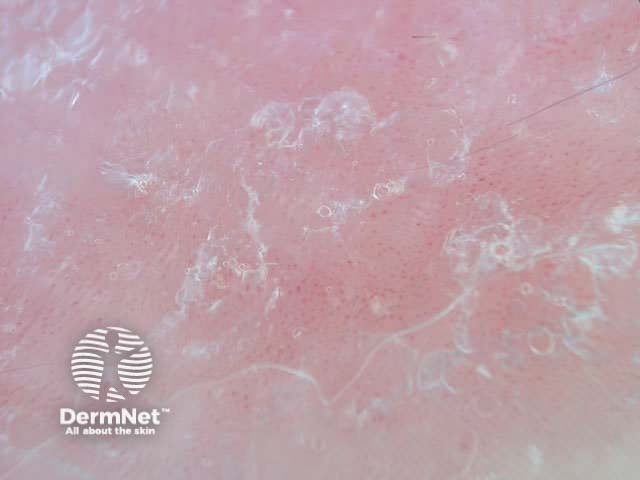
Dermoscopy of trichoepithelioma
Trichoepithelioma and trichadenoma are benign hair follicle tumours. Dermoscopy of these lesions usually shows multiple white clods of variable diameter ( milia like cysts ). This allows them to be distinguished from basal cell carcinoma on most occasions.

*Images supplied by Dr Mike Inskip
Inflammatory dermatoses
The vascular pattern seen on dermoscopy can be used to diagnose red scaly plaques:
- Amelanotic melanoma: atypical and polymorphous vascularity
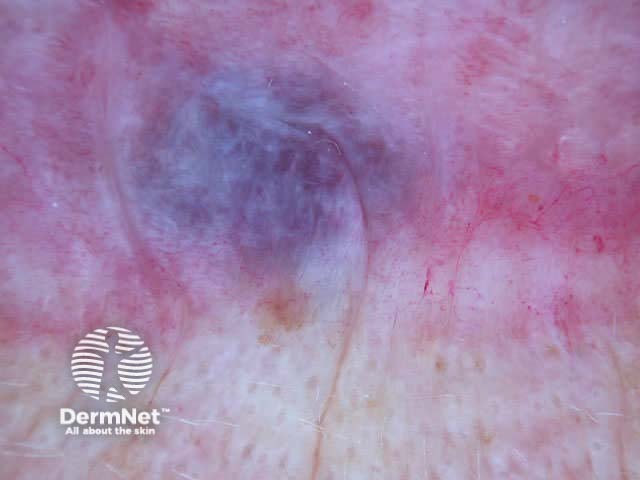
- Superficial basal cell carcinoma: arborising telangiectasia, ulceration
- Squamous cell carcinoma in situ: grouped glomerular vessels
- Psoriasis: uniform distribution of red dots on a light pink homogeneous background
- Lichen planus: white Wickham's striae, paucity of vessels



Skin infestations
Entodermoscopy is the use of dermatoscopy to:
- Identify a scabies mite and/or its faeces within its burrow. The head is triangle shaped on its back, and anchor shaped on its front, like a jet-plane.
- Confirm the presence of nits gripping a hair shaft in pediculosis capitis (a filled egg case has a dark tip and is bullet shaped; an empty one is transparent, and shorter with a flat top).
- Evaluate cutaneous larva migrans



Capillaroscopy
A dermatoscope can be used to evaluate capillaries. For example
- Cuticular capillaroscopy in suspected connective tissue disease.


Activity
How does nail fold capillaroscopy distinguish lupus erythematosus from systemic sclerosis?
References
- Zalaudek I, Argenziano G, Di Stefani A, Ferrara G, Marghoob AA, Hofmann-Wellenhof R, Soyer HP, Braun R, Kerl H. Dermoscopy in general dermatology. Dermatology. 2006;212(1):7-18. Medline.
- Arpaia N, Cassano N, Vena GA. Dermoscopic patterns of dermatofibroma. Dermatol Surg. 2005 Oct;31(10):1336-9. Medline.
- Zalaudek I, Ferrara G, Leinweber B, Mercogliano A, D'Ambrosio A, Argenziano G. Pitfalls in the clinical and dermoscopic diagnosis of pigmented actinic keratosis. J Am Acad Dermatol. 2005 Dec;53(6):1071-4. Medline.
- Felder S, Rabinovitz H, Oliviero M, Kopf A. Dermoscopic differentiation of a superficial basal cell carcinoma and squamous cell carcinoma in situ. Dermatol Surg. 2006 Mar;32(3):423-5. Medline.
- Zalaudek I, Argenziano G, Leinweber B, Citarella L, Hofmann-Wellenhof R, Malvehy J, Puig S, Pizzichetta MA, Thomas L, Soyer HP, Kerl H. Related Articles, Links Abstract Dermoscopy of Bowen's disease. Br J Dermatol. 2004 Jun;150(6):1112-6. Medline.
- Bergman R, Sharony L, Schapira D, Nahir MA, Balbir-Gurman A. The handheld dermatoscope as a nail-fold capillaroscopic instrument. Arch Dermatol. 2003 Aug;139(8):1027-30. Medline.
- Cheng ST, Ke CL, Lee CH, Wu CS, Chen GS, Hu SC. Rainbow pattern in Kaposi's sarcoma under polarized dermoscopy: a dermoscopic pathological study. Br J Dermatol. 2009 Apr;160(4):801-9.
- Huerta-Brogeras M, Olmos O, Borbujo J et al. Validation of dermoscopy as a real-time noninvasive diagnsotic imaging technique for actinic keratosis. Arch Dermatol 2012;148:1159-1161
On DermNet
- Skin lesions
- Dermatoscopy quizzes
- Dermatoscopy Information for patients
- Dermatoscope overview
- Image acquisition
Books about skin diseases
See the DermNet bookstore.